Back when I was at Google we had a phrase, “I don’t know how to count that low”. It was used to dismiss normal-company-sized problems as beneath our dignity to engage with: if you didn’t need 100 database shards scattered around the globe, were you even doing real work?
It was used as a sign of superiority within Google, but it also pointed at a real problem: I once failed a job interview at a start-up when I wondered out loud if the DB was small enough to be held in memory, when it was several orders of magnitude lower than when I should even have begun worrying about that. I didn’t know the limit because it had been many years since I’d had a problem that could be solved with a DB small enough to be held in its entirety in memory. And they were right to fail me for that: the fact that I was good at solving strictly more difficult problems didn’t matter because I didn’t know how to solve the easier ones they actually had. I could run but not walk, and some problems require walking.
It’s a problem, but it can be a pleasant kind of problem to have, compared to others. Another example: my dad is a Ph.D. statistician who spent most of his life working in SAS, a powerful statistical programming language, and using “spreadsheet statistics” as a slur. When I asked permission to share this anecdote he sent me a list of ways Excel was terrible.
Then he started consulting for me, who was cruelly unwilling to pay the $9000 license fee for SAS when Google Sheets was totally adequate for the problem (WHO HAS FOOD AT HOME NOW DAD?!?).*
My dad had to go through a horrible phase of being bad at the worse tool, and found a lot of encouragement when I reframed “I could have done this with one line in SAS and am instead losing to this error-riddled child’s toy” to “I didn’t know how to count that low, but now that it matters I am learning”. And then he tried hard and believed in himself and produced that analysis of that informal covid study that was wonderful statistically and super disappointing materially. And I retrained on smaller numbers and got that job at that start-up.
These are the starkest examples of how I’ve found “I don’t know how to count that low” useful. It reframes particularly undignified problems as signs of your capacity rather than incapacity, without letting you off the hook for solving them. Given how useful it’s been to me and how little I’ve seen of it in the wild, I’d like to offer this frame to others, to see if it’s useful for you as well.
*If any of you are going to bring up R: yes, it’s free, and yes, he has some experience with it, but not enough to be self-sufficient, I knew Sheets better, and I knew it was totally adequate for what we were doing or were likely to do in the future.
Appendix: I know you’re going to ask, so here is his abbreviated of grievances with Excel. Note that this was Excel in particular; I have no idea if it applies to Google Sheets. I also would allow that this must have been years ago and Excel could have gotten better, except AFAIK they never fixed the problem with reading genes as dates so they get no benefit of a doubt from me.
I attended a talk by a statistician at Microsoft. He said that Microsoft had decided that there was no competitive advantage in making Excel statistics better because no statistician used it for serious problems except for data entry, so:
1. he was the only statistician at Microsoft 2. he knew of seven serious statistical problems in Excel, but they wouldn’t give him the money to fix them. 3. Excel’s problems fell into two categories: 3a. terrible numerical analysis: it was widely verified if you took a number of single-digit numbers and calculated their standard deviation, and then took the same numbers and added a million to them, the standard deviation was often different, when it should be exactly the same. 3b.
statistical errors – like not understanding what you’re copying out of a textbook and getting it wrong.
Thanks to Ray Arnold and Duncan Sabien for beta-reading, and my dad for agreeing have his example shared.
A client came to me to investigate the effect of high altitude on child development and has given me permission to share the results. This post bears the usual marks of preliminary client work: I focused on the aspects of the question they cared about the most, not necessarily my favorite or the most important in general. The investigation stops when the client no longer wants to pay for more, not when I’ve achieved a particular level of certainty I’m satisfied with. Etc. In this particular case they were satisfied with the answer after only a few hours, and I did not pursue beyond that.
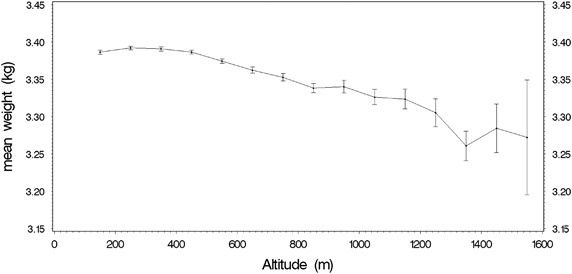
That out of the way: I investigated the impact of altitude on childhood outcomes, focusing on cognition. I ultimately focused mostly on effects visible at birth, because birth weight is such a hard to manipulate piece of data. What I found in < 3 hours of research is that altitude has an effect on birth weight that is very noticeable statistically, although the material impact is likely to be very small unless you are living in the Andes.
Children gestated at higher altitudes have lower birth weights
This seems to be generallysupported by studies which are unusuallyrigorous for the field of fetal development. Even better, it’s supported in both South America (where higher altitudes correlate with lower income and lower density, and I suspect very different child-rearing practices) and Colorado (where the income relationship reverses and while I’m sure childhoods still differ somewhat, I suspect less so). The relationship also holds in Austria, which I know less about culturally but did produce the nicest graph.
This is a big deal because until you reach truly ridiculous numbers, higher birth weight is correlated with every good thing, although there’s reason to believe a loss due to high altitude is less bad than a loss caused by most other causes, which I’ll discuss later.
[Also for any of you wondering if this is caused by a decrease in gestation time: good question, the answer appears to be no.]
Children raised at higher altitudes do worse on developmental tests
There is a fairamount of data supporting this, and some even attempt to control for things like familiar wealth, prematurity, etc. I’m not convinced. The effects are modest, I expect families living at very high altitudes (typically rural) to be different in many ways from lower altitudes (typically urban) in ways that cause their children to score differently on tests without it making a meaningful impact on their life (and unlike birth weight, I didn’t find studies based in CO, where some trends reverse). Additionally, none of the studies looked specifically at children who were born at a lower altitude and moved, so some of the effects may be left over from the gestational effects discussed earlier.
Hypoxia may not be your only problem
I went into this primed to believe reduced oxygen consumption was the problem. However, there’s additional evidence that UV radiation, which rises with altitude, may also be a concern. UV radiation is higher in some areas for other reasons, which indeed seems to correlate with reductions in cognition.
How much does this matter? (not much)
Based on a very cursory look at graphs on GIS (to be clear: I didn’t even check the papers, and their axes were shoddily labeled), 100 grams of birth weight corresponds to 0.2 IQ points for full term babies.
The studies consistently showed ~0.09 to 0.1 grams lower birth weight per meter of altitude. Studies showed this to be surprisingly linear; I’m skeptical and expect the reality to be more exponential or S shaped, but let’s use that rule of thumb for now. 0.1g/m means gestating in Denver rather than at sea level would shrink your baby by 170 grams (where 2500g-4500g is considered normal and healthy). If this was identical to other forms of fetal weight loss, which I don’t think it is, it would very roughly correspond to 0.35 IQ points lost.
However, there’s reason to believe high-altitude fetal weight loss is less concerning than other forms. High altitude babies tend to have a higher brain mass percentage and are tall for their weight, suggesting they’ve prioritized growth amidst scarce resources rather than being straight out poisoned. So that small effect is even smaller than it first appears.
There was also evidence out of Austria that higher altitude increased risk of SIDS, but that disappeared when babies slept on their backs, which is standard practice now.
So gestating in Denver is definitely bad then? (No)
There are a billion things influencing gestation and childhood outcomes, and this is looking at exactly one of them, for not very long. If you are making a decision please look at all the relevant factors, and then factor in the streetlight effect that there may be harder to measure things pointing in the other direction. Do not overweight the last thing I happened to read.
In particular, Slime Mold Time Mold has some interesting data (which I haven’t verified but am hoping to at least ESC the series) that suggests higher altitudes within the US have fewer environmental contaminants, which you would expect to have all sorts of good effects.
Yesterday* I talked about a potential treatment for Long Covid, and referenced an informal study I’d analyzed that tried to test it, which had seemed promising but was ultimately a let down. That analysis was too long for its own post, so it’s going here instead.
Gez Medinger ran an excellent-for-its-type study of interventions for long covid, with a focus on niacin, the center of the stack I took. I want to emphasize both how very good for its type this study was, and how limited the type is. Surveys of people in support groups who chose their own interventions is not a great way to determine anything. But really rigorous information will take a long time and some of us have to make decisions now, so I thought this was worth looking into.
Medinger does a great analysis in this youtube video. He very proactively owns all the limitations of the study (all of which should be predictable to regular readers of mine) and does what he can to make up for them in the analysis, while owning where that’s not possible. But he delivers the analysis in a video rather than a text post ugh why would you do that (answer: he was a professional filmmaker before he got long covid). I found this deeply hard to follow, so I wanted to play with the data directly. Medinger generously shared the data, at which point this snowballed into a full-blown analysis.
I think Medinger attributes his statistics to a medical doctor, but I couldn’t find it on relisten and I’m not watching that damn video again. My statistical analysis was done by my dad/Ph.D. statistician R. Craig Van Nostrand. His primary work is in industrial statistics but the math all transfers, and the biology-related judgment calls were made by me (for those of you just tuning in, I have a BA in biology and no other relevant credentials or accreditations).
The Study
As best I can determine, Medinger sent a survey to a variety of long covid support groups, asking what interventions people had tried in the last month, when they’d tried them, and how they felt relative to a month ago. Obviously this has a lot of limitations – it will exclude people who got better or worse enough they didn’t engage with support groups, it was in no way blinded, people chose their own interventions, it relied entirely on self-assessment, etc.
Differences in Analysis
You can see Medinger’s analysis here. He compared the rate of improvement and decline among groups based on treatments. I instead transformed the improvement bucket to a number and did a multivariate analysis.
Much better (near or at pre-covid)
1
Significantly better
0.5
A little better
0.1
No change
0
A little worse
-0.2
Significantly worse
Curiously unused
Much worse
-1.2
You may notice that the numerical values of the statements are not symmetric- being “a little worse” is twice as bad as “a little better” is good. This was deliberate, based on my belief that people with chronic illness on average overestimate their improvement over short periods of time. We initially planned on doing a sensitivity analysis to see how this changed the results; in practice the treatment groups had very few people who got worse so this would only affect the no-treatment control, and it was obvious that fiddling with the numbers would not change the overall conclusion.
Also, no one checked “significantly worse”, and when asked Medinger couldn’t remember if it was an option at all. This suggests to me that “Much worse” should have a less bad value and “a little worse” a more bad value. However, we judged this wouldn’t affect the outcome enough to be worth the effort, and ignored it.
We tossed all the data where people had made a change less than two weeks ago (this was slightly more than half of it), except for the no-change control group (140 people). Most things take time to have an effect and even more things take time to have an effect you can be sure isn’t random fluctuation. The original analysis attempted to fix this by looking at who had a sudden improvement or worsening, but I don’t necessarily expect a sudden improvement with these treatments.
We combined prescription and non-prescription antihistamines because the study was focused on the UK which classifies several antihistamines differently than the US.
On row 410, a user used slightly nonstandard answers, which we corrected to being equivalent to “much improved’, since they said they were basically back to normal.
Medinger uses both “no change” and “new supplements but not niacin” as control groups, in order to compensate for selection and placebo effects from trying new things. I think that was extremely reasonable but felt I’d covered it by limiting myself to subjects with >2 weeks on a treatment and devaluing mild improvement.
Results
I put my poor statistician through many rounds on this before settling on exactly which interventions we should focus on. In the end we picked five: niacin, anti-histamines, and low-histamine diet, which the original analysis evaluated, and vitamin D (because it’s generally popular), and selenium (because it had the strongest evidence of the substances prescribed the larger protocol, which we’ll discuss soon).
Unfortunately, people chose their vitamins themselves, and there was a lot of correlation between the treatments. Below is the average result for people with no focal treatments, everyone with a given focal treatment, and everyone who did that and none of the other focal treatments for two weeks (but may have done other interventions). I also threw in a few other analyses we did along the way. These sample sizes get really pitifully small, and so should be taken as preliminary at best.
Treatment
Niacin, > 2 weeks
Selenium, > 2 week
Vitamin D, > 2 week
Antihistamines, > 2 weeks
Low-histamine diet, > 2 weeks
Change (1 = complete recovery)
95% Confidence Interval
n
No change
0
0
0
0
0
0.04
± 0.07
140
Niacin, > 2 weeks
1
–
–
–
–
0.23
± 0.07
91
Selenium, > 2 weeks
–
1
–
–
–
0.24
±0.07
88
Vitamin D, > 2 week
–
–
1
–
–
0.15
±0.05
261
Antihistamines, >2 weeks
–
–
–
1
–
0.18
± 0.06
164
Low histamine diet
–
–
–
–
1
0.18
±0.06
195
Niacin, > 2 weeks, no other focal treatments
1
0
0
0
0
0.15
±0.2
11
Selenium, > 2 weeks, no other focal treatments
0
1
0
0
0
0.05
±0.06
4
Vitamin D, > 2 week, no other focal treatments
0
0
1
0
0
0.07
±0.08
106
Antihistamines, >2 weeks, no other focal treatments
0
0
0
1
0
0.08
±0.13
26
Low histamine diet, > 2 weeks, no other focal treatments
0
0
0
0
1
0.13
±0.14
44
All focal treatments
1
1
1
1
1
0
Niacin + Antihistamines, >2 weeks
1
–
–
1
0
0.33
± 0.07
38
Niacin + Low Histamine Diet, > 2 weeks
1
0
0
0
1
0.29
±0.10
36
Selenium + Niacin, no histamine interventions
1
1
–
0
0
0.05
±0.19
17
Niacin, > 2 weeks, no other focal treatments, ignore D
1
0
–
0
0
0.13
±0.12
19
Selenium, > 2 weeks, no other focal treatments, ignore D
0
1
–
0
0
0.16
±0.12
18
1 = treatment used
0 = treatment definitely not used
– = treatment not excluded
Confidence interval calculation assumes a normal distribution, which is a stretch for data this lump and sparse but there’s nothing better available.
[I wanted to share the raw data with you but Medinger asked me not to. He was very fast to share with me though, so maybe if you ask nicely he’ll share with you too]
You may also be wondering how the improvements were distributed. The raw count isn’t high enough for really clean curves, but the results were clumped rather than bifurcated, suggesting it helps many people some rather than a few people lots. Here’s a sample graph from Niacin (>2 weeks, no exclusions)
Reasons this analysis could be wrong
All the normal reasons this kind of study or analysis can be wrong.
Any of the choices I made that I outlined in “Differences…”
There were a lot of potential treatments with moderate correlations with each other, which makes it impossible to truly track the cause of improvements.
Niacin comes in several forms, and the protocol I analyze later requires a specific form of niacin (I still don’t understand why). The study didn’t ask people what form of niacin they took. I had to actively work to get the correct form in the US (where 15% of respondents live); it’s more popular but not overwhelmingly so in the UK (75% of respondents), and who knows what other people took. If the theory is correct and if a significant number of people took the wrong form of niacin, it could severely underestimate the improvement.
This study only looked at people who’d changed things in the last month. People could get better or worse after that.
There was no attempt to look at dosage.
Conclusion
For a small sample of self-chosen interventions and opt-in participation, this study shows modest improvements from niacin and low histamine diets, which include overlap with the confidence interval of the no-treatment group if you exclude people using other focal interventions. The overall results suggest that either something in the stack is helping, or that trying lots of things is downstream of feeling better, which I would easily believe.
Thank you to Gez Medinger for running the study and sharing his data with me, R. Craig Van Nostrand for statistical analysis, and Miranda Dixon-Luinenburg for copyediting.
* I swear I scheduled this to publish the day after the big post but here we are three days later without it unpublished, so…
This article contains an interview with a doctor who believes NAD+ is the secret to covid’s heavy morbidity and mortality toll. The description was unusually well done for internet crackpottery. This is hard to convey rigorously, but it had a mechanistic-ness and the right level of complexity about it, and it made the right level of promises for a treatment. None of this is to say it’s definitely correct, but it had a bunch better chance of being correct than your average alt-covid-cure scribbled out in crayon. So I did some checks on it.
[Didn’t you say the risk of long covid was small? NO I SAID IT WAS TOO SMALL TO MEASURE AGAINST THE DELUGE OF CRAP THAT HAPPENS TO US EVERYDAY THAT IS NOT THE SAME]
*ahem*
This post is organized as follows:
Description of theory.
Long section defining terms. These are all useful for understanding the claims I check later on, but depending on who you are they may not be helpful, and you may find the contextless infodump kind of a drag. Feel free to skip if it’s not useful to you personally, and know that it’s there if you need it.
Deep dive onto particular claims the article makes.
Does it work?
Is it safe?
My personal experience with the protocol
Some meta
This is your reminder that my only credential is a BA in biology and I didn’t specialize in anything relevant. It is a sign of civilizational inadequacy that this post exists at all, and you should think really hard and do your own research before putting too much weight on it.
For those of you would like to skip to the take home message: science is very hard, I’m glad they’re running larger studies to follow up on all of these because that’s a reasonable thing for a rich society to do, but I’m not super hopeful about this protocol.
The Theory
As described by Dr. Ade Wentze:
There is an extremely widely used coenzyme in your body, NAD. The more active form of this compound, NAD+, is depleted by covid (converted to NADH). In people with a preexisting deficiency or difficulty rebounding after depletion, covid infection results in a persistent NAD+ deficit. This is bad in and of itself, but causes additional problems when your body tries to make up for it by requisitioning all your tryptophan to make more. Tryptophan is also a precursor for serotonin, so this leads to either low serotonin or activation of mast cells to release their serotonin stores, accompanied by histamines (which cause allergies and other issues).
Background
There is a lot of vocabulary in that theory and in the supporting claims, which I go over here. If you’re reading for conclusions rather than deep understanding I would skip this.
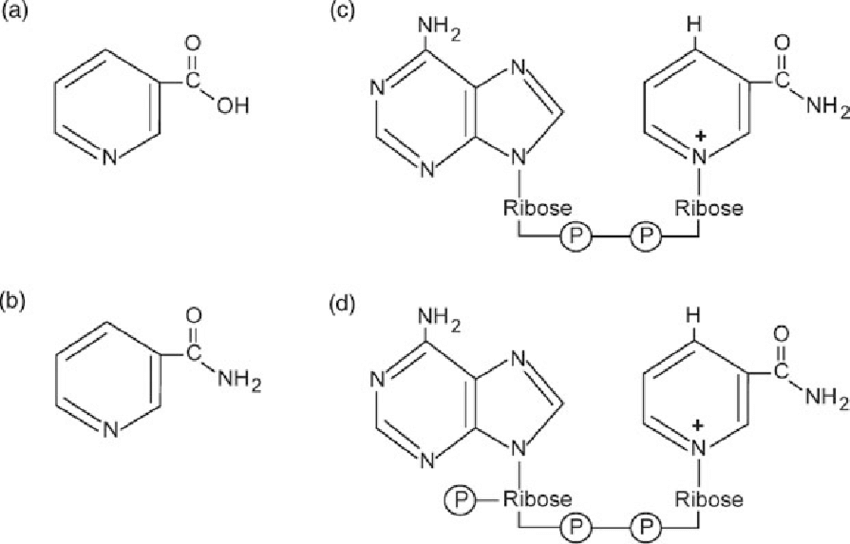
NAD+
Nicotinamide adenine dinucleotide is a coenzyme that plays an essential role in hundreds of chemical reactions in your cells, including many relating to processing energy and genetic transcription. This is a mixed blessing as a foundation for crackpot theories go: something involved in hundreds of processes across every kind of tissue in your body can cause almost any symptom, which is great because long covid has a lot of symptoms to cover. On the other hand, it can cause almost any symptom, which means it’s hard to disprove, and you should distrust things in proportion to the difficulty to disprove them. Alas, sometimes core processes are impaired and they do express that impairment in a range of unpredictable ways that vary across people, but it’s also an easy home for crackpots.
NAD+ has two major components, one made from either tryptophan or aspartic acid (both amino acids), or by altering niacin.
Niacin
Like many vitamins, niacin aka vitamin B3 refers to a few different closely related compounds (most commonly nicotinic acid, nicotinamide, nicotinamide riboside, and inositol nicotinate, but there are others) that are almost but not quite interchangeable.
Niacin is commonly prescribed for treating high cholesterol, although a metareview found it did not reduce overall mortality and may contribute to the development of type-2 diabetes.
Severe niacin deficiency is called pellagra, and can be caused by either insufficient consumption or problems processing the vitamin. Pellagra is mostly defined as niacin deficiency but can also be caused by tryptophan deficiency, which you may remember is another path to manufacturing NAD+. Pellagra can cause diarrhea, dermatitis, dementia, and death, which are not a great match for acute or long covid. Niacin supplementation treats pellagra, often within a few days.
SIRT1
Sirtuin 1, also known as NAD-dependent deacetylase sirtuin-1, is a protein that regulates the expression of some genes in ways that haven’t yet been made clear to me but seem to be associated with aging (more SIRT1 is associated with better outcomes, although we haven’t broken down cause and effect). As indicated by its name, it’s dependent on NAD+ to operate, which means NAD+ is involved in the regulation of expression of some genes via some mechanism, which means niacin is involved in the regulation of expression of some genes via some mechanism.
SIRT1 is downregulated in cells that have high insulin resistance and inducing its expression increases insulin sensitivity, suggesting the molecule is associated with improving insulin sensitivity.
Another many-purposed enzyme whose activities include DNA repair, killing cells that are beyond repair. PARP requires NAD+ as a coenzyme.
Individual Claims
Groups with low NAD+ suffer more from covid
NAD+ declines with age
NAD+ does definitely decline with age but so does literally everything bad in your body, so I don’t find this very compelling.
Correlation between NAD+ levels and Age in (A) Males (B) Females (source)
Obese people have lower NAD+ levels, leading to worse outcomes
Yes, although obese people tend to do worse on a lot of metrics. However, that paper highlights that SIRT1 seems to be involved in this correlation somehow.
Diabetics have worse NAD+ levels
Yes, although diabetics also have more immune problems generally (definitely Type 2, some pop sites said the same for Type 1 and that’s believable but I didn’t quickly find a paper I liked that backed the claim).
Low selenium is associated with bad outcomes in covid
The post cites Zhang et al, which took advantage of high variations in selenium consumption in China to do a natural experiment. Variations in the population selenium levels do seem insanely correlated with the overall cure rate (defined as not dying). The study took place in February 2020 so neither data collection nor treatment was very good, but damn that is interesting.
Moreover, this study, which came out several months after the blog post was published, took advantage of the same variation and came to the same conclusion, with a much larger sample size and much more reasonable case fatality rate (1.17% in areas with no deficiency to 3.16% in severely deficient areas, P = 0.002). (Note: several authors on that paper are also named Zhang, but I assume that’s because it’s a common name in China).
Some pharma company thinks selenium is promising enough to launch a trial for it, although recruitment hasn’t started yet.
The pre-print servers are littered with natural experiments highlighting correlations that failed as interventions, but this is very strong for a correlation.
Niacin just generally seems to help lung damage
That is indeed what their citation says, however that paper’s only source looked at the effect of niacin on lung damage in hamsters deliberately induced with a chemotherapy drug, and it’s not obvious to me that that translates to damage from infection or immune reaction. There are some other scattered studies in rodents, combining niacin with other substances, none of which looked at damage from infectious disease.
The treatment for NAD+ deficiency is niacin
Their citation backs this up: niacin supplementation led patients (n=5) and controls (healthy people given the same supplementation, n=8) to increased NAD+ levels, and arguably increased strength, although with that much variation and such a small sample size I’m not convinced. Martens et al supports this with modest benefits seen in n=24 subjects.
A few minutes investigation found some other studies:
Dietary niacin deficiency led to NAD+ deficiency in baby rats. This paper works damn hard to hide its sample size but I think it was 10-15 per treatment group.
The same author exposed some rats (n=6 per treatment group) to excess oxygen and found that those with a niacin deficient diet had less NAD+ in the lungs and responded less to the damage caused by excess oxygen, but had the same wet/dry ratio as their well-fed friends (wet/dry ratio is a measure of lung health).
Ng et al found that in catfish liver NAD increased linearly with dietary niacin supplementation, but health returns like size and mortality dropped off between 6 and 9 mg/kg. They further found that tryptophan supplementation could not make up for a niacin deficiency (in catfish).
Plus niacin is so well established as a treatment for pellagra that no one bothers to cite anything for it, and that does seem to mediate through NAD+.
Nicotinic acid may act as a one of a kind bioenergetic “pump” of inflammatory molecules out of cells
They link to a preprint which has since been taken down, and I could not find it on my own.
NAD+ problems have been indicated in chronic fatigue syndrome
Everything has been indicated in chronic fatigue syndrome; I’m not looking this up.
Mast cells indeed produce serotonin, in mice. Note that that paper highlights fluoxetine as a way to reverse serotonin deficiency in mast-cell-deficient mice, and since the article was published fluoxetine has shown promise as a covid treatment. However this study says that while serotonin-producing mast cells are common, humans in particular don’t have them while healthy (although it still shows serotonin affecting mast cell movements). This appears to be an area of some controversy.
Mast cells releasing histamine in response to allergens is uncontroversial. Moreover, histamines and serotonin are stored in the same compartments (in mice). Second source (still in mice).
Some Guy did an informal study based on this theory and it worked
Some guy (Birth name: Gez Mendinger) did indeed report this, and I have to say, for an uncredentialed dude on youtube recommending OTC supplements to treat a nebulously defined disease, this guy looks really credible, and his reasonably good analysis was quite promising. He shared his results with me, and it continued to look promising when I first dug into it with assistance from a statistician, but the deeper we drilled the less promising it looked (details). By the end, the most I could say is “yeah, worth a harder look”, but the history of things that look promising in small, poorly organized studies that wilt under large, well-organized ones is just too dismal to ignore.
Mouse study shows low NAD+ hurts you via SIRT1
The interview also cites this mouse study featuring a direct NAD+ drip and a slightly different coronavirus. They show improved symptoms but not viral load. They don’t list the sample size anywhere I can find, judging from the low-resolution graph it looks like 7 mice in the control group and maybe 12 in the treatment group? Except for the embolism test which had many more mice.
(apologies for poor image quality, the PDF was crap)
(note: that article was up when I started this post but disappeared before I verified the SIRT1-specific part of the claim)
Quercetin increases NAD+ levels
Yes, in rats and mice. Specifically, it speeds up the transition from NADH to NAD+
Male pattern balding and low vitamin D are both associated with poor covid outcomes and low NAD+.
The balding citation does indeed say that, but it only looked at hospitalized patients so it’s useless. Moreover, balding is associated with a testosterone derivative, and testosterone weakens the immune system. But when I went to find some cites for those, I found that within hospitalized patients, low testosterone was associated with worse outcomes. However these patients were already hospitalized, so the causality could easily go the other way.
Meanwhile I found severalfolk-wisdomlevel comments indicating a link between NAD+ and male pattern balding, but nothing rigorous.
Low vitamin D does seem to be associated with poor covid outcomes, maybe, but treatment doesn’t seem to help (at least not if you wait until patients are hospitalized).
Chang and Kim assert that Vitamin D activates the NAD-SIRT1 pathway in fat cells in vitro, which if it held up elsewhere would be even stronger evidence for the overall theory than this claim attempts. Byers et al found that vitamin D did not protect guinea pigs against the NAD+ depleting effects of mustard gas. This is not a slam dunk.
Covid depletes NAD+ by activating PARP
Curtin et al lay out a theoretical case for using PARP-inhibitors to treat covid-caused ARDS.
Heer et al “we show that SARS-CoV-2 infection strikingly upregulates MARylating PARPs and induces the expression of genes encoding enzymes for salvage NAD synthesis from nicotinamide (NAM) and nicotinamide riboside (NR), while downregulating other NAD biosynthetic pathways” (notably, the forms not used in the protocol), “overexpression of PARP10 is sufficient to depress cellular NAD and that the activities of the transcriptionally induced enzymes PARP7, PARP10, PARP12 and PARP14 are limited by cellular NAD and can be enhanced by pharmacological activation of NAD synthesis”, “MHV induces a severe attack on host cell NAD+ and NADP+.” (MHV being used as a model)
Long covid and Pellagra share a lot of symptoms, including hyponosmia
Scatteredclaims pellagra causes hyponosmia but you have to look really hard, it doesn’t show up on any of the common descriptions. I checked in Spanish and didn’t find anything either.
Sen (published only last month) suggests that serotonin deficiency causes anosmia and other neuro symptoms in covid. They propose a different method for the depletion (ACE2 is a mechanism for moving serotonin into the cell), but it’s not mutually exclusive with Wentzel’s theory (that NAD+ depletion causes the body to use up tryptophan trying to produce more NAD+).
Your body hijacks tryptophan to make NAD+ at the expense of serotonin
Tryptophan can indeed be used to make NAD (albeit niacin is better) and serotonin. How your body prioritizes under a given set of circumstances is anyone’s guess.
NAD+ and the immune system
Probably at least some of long covid stems from autoimmune issues, as witnessed by the fact that it’s much more common in women and sometimes helped by steroids. The post and paper don’t make any claims on this beyond the effect of NAD+ on mast cells, which are implicated in autoimmune disorders, but out of curiosity I did some quick googling and found that NAD+ downregulate inflammation via CD4 cells (in mice) and activating SIRT1, the pathway mentioned previously (still in mice).
Not that good. Feels associational rather than mechanistic. However Bordoni et al (published after the cited paper) found covid-19 was associated with diminished SIRT1- but Pinto et al found covid-19 upregulated SIRT1 and cite another study claiming that under conditions of energetic stress (which would imply low NAD+), SIRT1 substitutes for ACE2 (the receptor covid uses to enter the cell. Smith suggests that downregulating SIRT1 is good for fighting covid. So SIRT1, NAD+, and covid are probably related, but the first two items are very common so this isn’t damning.
Notably, this paper doesn’t explain why covid would deplete NAD+ more than other infectious diseases, which is an enormous hole.
Does it work?
The mechanism and empirical data are definitely enough to merit more rigorous follow-up studies (which are in progress) and definitely not slam dunks. But you may need to make a decision before that’s in, so the real question is “should I take this stack if I get sick? Should my parents?”
My tentative answer is: the prescribed stack probably won’t physically hurt you (but see the next section), and it’s fairly cheap, so the limiting factor is probably “what do you have the energy to try”. This is a better thing to try than the interventions whose proof was actively made up or have been investigated and discarded, but there undoubtedly are or will be equally probable things floating around, and choosing between them will be a matter of taste..
If you do end up giving this a shot, for covid long or acute, I invite you to preregister your complaints and intention with me (a comment here or email elizabeth@acesounderglass.com), so I can create my own little study. If you don’t feel like doing that I still encourage you to announce the intention somewhere, as a general good practice (I did so here).
So you’re saying it’s safe then?
Anything that does anything is dangerous to you in sufficient dosages. If you’re considering an unverified supplement stack, you should carefully investigate the potential side effects of each substance and consider it in light of what you know of your own health (especially other medications you’re taking). Consider talking to a doctor, if you have a good one.
If any of you are thinking “oh niacin’s a water-soluble vitamin it must be fine”: that’s a pretty good heuristic but it doesn’t hold for niacin in particular.
My experience
As mentioned previously, I acquired lingering progressive chest congestion/inflammation from (probably) my covid vaccine. It’s always possible there was another reason but the timing and symptoms really do not match anything else.
Since I never had covid (probably), my reaction can’t come from the infection itself, only my immune response to it. Since the theory doesn’t specify a mechanism that’s not disqualifying, but they do make it sound like it starts as a covid problem not an immune problem.
I started this supplement stack before doing any deep verification. The original blog post pattern matched to the kind of thing that was worth trying, everything on the list I either knew was generally safe or confirmed with a quick check (my doctor later confirmed my opinion on safety without endorsing the stack for any particular use), and I had a lot of client work to do. Shoemaker’s children go barefoot, and all that. So by the time I was writing this I had been on the recommended supplement stack (and some other things besides) for 3 weeks, and was beginning to wean down.
Overall: my chest pain got better but the timing fits better with attribution to a different intervention. The rash I got on matches very well with the supplement stack. I nonetheless was craving it after I weaned off, so probably there’s at least one thing in it I need, which hopefully isn’t the same as the thing causing the rash.
[Alert twitter readers may have questions, since I previously was more positive on the stack. I had a major regression when I got a non-covid cold, and had to go back on the other treatment]
Interestingly, my tolerance for niacin increased and then plummeted. Originally I could take 250mg (the smallest size I could find in the right form) with only very mild flush, and that got better over time, to the point I tried 500 mg once (a mistake). But around week 3 my flush was getting worse. Lowering the dose helped, but it’s getting worse again, so I’m continuing to titrate down. This is extremely consistent with filling up NAD+ reserves over time, although very far from conclusive.
Meta
I was originally much more positive on this treatment/theory. I gave it more credit on Twitter, but that’s nothing compared to the excited messages I sent a few friends after an initial lit review. I wrote several much more positive versions of this post (and the forthcoming study analysis), but there kept being one more thing to check, until I talked my way down to what you see here. Some of my downgrade stemmed from asking better statistical questions, but some of it was just the emotional process of talking myself down from something that initially looked so promising, but ultimately had a similar amount of holes to many other things that looked equally promising and failed to pay off. This represents dozens of hours of work from me and my statistician, for the very disappointing result of “fringe treatment probably doesn’t do very much but can’t rule it out”. Reality is infinitely disappointing.
Thanks to Alex Ray and my Patreon Patrons for partially funding this investigation, and Miranda Dixon-Luinenburg for copyediting.