I never did do much with the kitten pain scale, because the pain meds’ effects were so striking there was no need for hour by hour monitoring. But I’ve found another good marker.
When I first started at crisis chat I really really loved it, and would frequently stay hours past my scheduled shift. I often left feeling energized*. At some point that changed. I put it down to a loss of novelty, or maybe nostalgia making me remember it as more fun than it was. I kept going because it wasn’t about me having fun, it was about me helping people, but I was more conservative about the latest time I would start a new chat.
Then I got those really awesome pain meds in January, and suddenly I was staying late again. But at some point it disappeared again.
One of the nice things about the meds is that they have a long lasting effecting. They push the pain-tension cycle back, so I’m in less pain for days or even weeks after they wear off. One of the bad things about one of them is that I hate being touched the next day. That’s suboptimum on its own, but it scares me to think of what else it’s doing that I’m not noticing, so I try to go as long as possible without taking it. I’m also very good at pushing away conscious knowledge of pain, even though it still effects me. So I ended up going really way too long without taking the topical pain medication.
Finally I took it again, and what do you know, I stayed more than two hours past the end of my next chat shift.
It doesn’t surprise me that I’m better at chatting when I’m in less pain, but I am surprised by the way I’m better. Ending chats is a tricky business. You don’t want people to feel shoved out the door, but a good chunk of our target audience is having anxious ruminations. The last two times I’ve been much better about recognizing when we’ve reached the end of the productive portion of the chat and wrapping it up. A few people even seemed to take the nudge out as permission to relax.
*although not always. Most days I had to call a child abuse report in were bad days
**Shift end times are a little fuzzy because of course you can’t leave in the middle of a chat. If it’s 5 minutes before your shift ends, of course you don’t take a new chat unless you’re prepared to stay late. But if it’s 30-45 minutes? You’ll probably be done only a little after your stated end, but you never know which call is going to be a two hour active rescue.
Left untreated, people with phenylketonuria (PKU) can develop intellectual disabilities, seizures, and “other medical problems”. But PKU does not cause any of those. Phenylketonuria + a normal diet causes a build of of phenylalinine in the body, which causes those problems. If PKU is caught at birth and the sufferer is kept on a phenylanlinine-light diet, they will never develop these problems.
Henry Markram suggests that something analogous is going on with autism. He and his collaborators think that the actual problem is that autistic babies have extraordinary sensory sensitivity, and this sensitivity causes defenses that cause them to miss certain critical information during developmental periods. What is challenging but achievable (the zone necessary for learning) for other people is overwhelming for them, so they don’t learn. The developmental window closes and they’ve lost their chance to truly master that skill. But if they were given stimulus in their zone of achievable challenge, they would learn those skills and maintain them for life. They might continue to need accommodations, the way phenylketonurics need to stay on a phenylalinine-light diet their whole life, but with those accommodations they could function “normally”. This is known as the intense world hypothesis.
The example they give is the critical period for learning language. You *can* learn a new language after the critical period, but it will never be as easy, most people will never attain genuine fluency, and if you never learn any language it may be truly impossible to pick one up later. If normal human speech is overwhelming to an autistic infant they will miss that period and their language will be impaired for life. But if they’re given regular access to speech they are comfortable with (probably quieter and slower) they could learn it just fine, the same way hearing impaired children do fine with sign language.
I was also really impressed with the writing of this lay-press article. I’ve been avoiding doing take downs, especially of popsci articles, because there are millions of wrong things every day and criticizing them is easy. For a while I could justify them as case studies in critical reading, but now it just feels bad. This had led to a lot of aborted blog entries, as I read something amazing and then realize it’s too flawed to pass on uncritically. I don’t agree with everything the article says (insisting there’s only one cause of autism strikes me less as brave and more as idiotic), but it lays out its case in an informative and responsible manner.
I jokingly referred to pain-induced ADD on Monday, but I’m becoming more and more convinced that is actually what was happening. After prior surgeries I was too exhausted to notice anything, but this time I was energetic enough to experience the pain. I mean, unless I tried to go outside or something. That led to a really entertaining systems crash in the supermarket. But if I stayed inside I was able to do things like get food and put away dishes without strain. Contrast with when my pain meds sabotaged my cortisol production. Intellectually I was there and able to do things like read and blog, but physically it was a struggle to make myself a smoothie.
After surgery I could not read or write or even enjoy a movie. It was more than pain making everything 70% less fun, it was that everything was annoying and frustrating and no fun at all. I couldn’t enter a state of flow or concentration or even relaxing for any length of time. Except when I played video games or the piano. Neither were fun, exactly, and I was still in pain, but they were at least distracting and rewarding. Looking back, this explains a lot of my behavior when I was in constant pain last year, it just took being out of pain and then very sharply in a lot of pain to make the pattern obvious.
At first I thought this was Harrison Bergeron type thing, where pain was sending out interrupts too often for me to get into a groove on anything. But then I read this blog post (blogs were just about in my power) by Sara Constantin on dopamine, explaining Peter Redgrave’s hypothesis that the spike (phasic increase) of dopamine is not itself a reward (which is how pop journalism usually describes it) but a timestamp that lets you know what actions should get credit for the actual reward chemicals you are about to receive. That would explain why humans and animals with broken dopamine systems do feel pleasure when eating but will nonetheless starve to death unless you put the food directly in their mouth.
Many of the drugs used to treat ADHD inhibit dopamine reuptake, which raises your tonic (baseline) dopamine levels. Constantin hypothesizes that if the baseline is too low than stimuli that should be ignored suddenly are interpreted as important, leading to a lot of SQUIRREL.
[ I was going to make this a gif but putting unpausable moving pictures in a post on ADHD just seemed cruel]
If this is correct, it offers an explanation for why ADHDers are so drawn to things like videogames and sex: the time gap between doing the correct thing and getting the chemical reward is so short they can still determine causality, even against the a background of SQUIRRELs. This needn’t be purely about hedonism- if it was, something consistently pleasant would work. I think it’s about having an internal locus of control and self-efficancy. Humans are happiest they feel like they have the power to change their own circumstances and have an impact on the world. It’s hard to feel those things if your attention is constantly being torn away from what you choose and you can’t (on a neural level) determine what made you feel the emotion you are currently feeling. This is one reason the toll of ADHD shouldn’t be measured in lost productivity alone; even people with very successful coping mechanisms are being denied that internal locus of control, and that’s miserable.
Here’s my contribution: my description of being in pain sounds a lot like other people’s description of ADHD, right down to video games being rewarding without strictly being fun. And as it turns out the basal ganglion, the area Redgrave believes is using dopamine to timestamp causes so they can be matched with effects, also releases dopamine in response to pain. It seems entirely possible to me that high baseline levels of dopamine could diminish the effect of a spike. Instead of everything being timestamped “good job”, nothing is, with similar results
But let’s make it even more interesting. Several anti-depressants are also useful in treating chronic pain, and NSAIDS (usually mild pain killers) treat depression. I had previously put this down to “pain is depressing”, “depression appears to be connected to inflammation in ways we don’t understand” and plain old “brains are squishy and they don’t make sense”, but if there was a causal link? The symptoms of depression include fatigue, feelings of helplessness and lost of interest or enjoyment of previously liked activities, which sure sounds related. Quick googling found a very tiny study showing a connection between low dopamine and suicide, and this fascinating study suggesting that inflammation reduced the basal ganglia’s production of dopamine, which would tie all of this up in a very pretty bow. Something causes pain and/or inflammation (the two often go together), which long term causes inflammation in the basal ganglia, which causes depression and reduces your body’s natural analgesics.
Look body, if you were worried about us getting high off of pain, maybe you could have releases fewer happy chemicals in response to pain, instead of making it just as fun but also cause depression some time later.
This would also explain why ADHD medicines are promising in treating depression (source, source, and a large showing among my friends), and why ADHD and depression so often go together.*
I cannot stress enough how unqualified I am to make this hypothesis. Lots of people know lots more on all of these things than me. But it comes together to be an extremely plausible explanation for both the literature I’ve read and my personal experiences.
*There’s a lot of evidence that depressed parents correlate with ADHD kids, but it’s probably environmental.
A new study by Reid et al claims to demonstrate a biological marker for the presence of depression. First we have the boring criticisms, like “32 is not a real sample size, “shotgunning 20 RNA markers and noticing which ones were increased in depressed patients and decreased after treatment is painting the target after you shot the gun” and “you’re comparing treatment group re-draws to control group baseline draws” but anyone could make those. The authors make several of those points themselves. And there are some statistical criticisms that pretty much invalidate the whole thing.* What I find interesting is that even if the results are correct, they may not be useful.
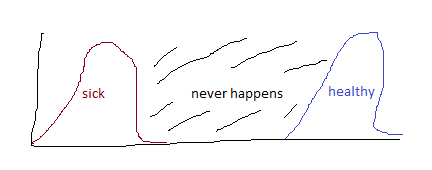
If you look at the table comparing the marker rates in depressed and non-depressed patients, there are 9 markers that differ in a statistically significant way. The problem is that they’re still not very far apart. What you would ideally like to see in a diagnostic test is the following:
Two bell curves with no overlap
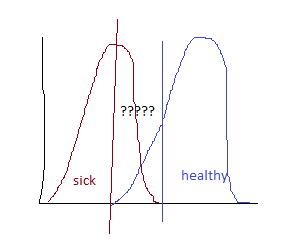
because then it easy to translate a test score into a health status. But the markers in this study are more like
two overlapping bell curves
Which means that if you know someone is depressed you can generate a pretty good idea of their marker score, but there’s a wide range where knowing their marker score doesn’t give you a good idea if they’re depressed. That makes it pretty useless for a screening test.
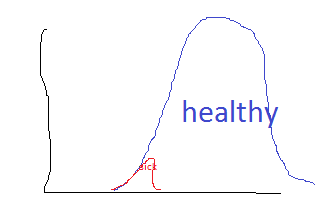
But it’s actually worse than that. There are many more undepressed people than depressed people, so the curves could look more like
Under this graph, the sick mean could be four standard deviations out from the health mean, and yet a person with a low marker score is approximately equally likely to be depressed or not. This is a bayesian reasoning problem and doctors are frighteningly bad at those, but then, they’re worse than chance at frequentist statistics too.
In summary, I’m not hopeful this proves to be a useful screening tool for depression.
*They don’t actually prove that the marker values of cured people converge with those of never-depressed people, they just fail to prove they’re statistically different. Those are different things. They also switch between two (equally valid) statistical tests (T-test and Fischer’s) without saying why, which means there is a high probability the answer is “we liked those answers more.”
[Had more dental surgery this week and am currently suffering from pain-induced ADD. Expect less research and more wild speculation]
Consider pre-emptive testing for psychiatric or developmental issues in children. If you’re too aggressive, you end up misdiagnosing a lot of perfectly normal deviations from the exact median as development issues in need of treatment. Development is complicated, different systems come on line at different rates and in different orders in different kids, and they should be allowed to do that without being corralled into fitting a predetermined schedule .
But if you’re not aggressive enough, the kids develop coping mechanisms that hide the disability, making it harder to diagnose and treat. Sometimes people treat this as solving the problem (especially for conditions that are often conflated with character flaws, like ADHD or some forms of depression), but they are wrong. At best lack of treatment holds people back from their true potential, at worst it twists up their internal structure in ways that break at the worst possible time (usually grad school). It’s a big problem with twice exceptional children, who have both brain-based deficiencies and a lot of raw intelligence, and I suspect for people with atypical presentations of their disabilities. E.g. girls with ADHD or autism spectrum issues, boys with depression* or trauma from sexual abuse.**
Even perfectly accurate testing won’t fix this, because developmental asynchronies do not necessarily indicate a future problem, and treating them can prevent the issue from fixing itself. The real issue is distinguishing natural, healthy leveling out from the development of costly compensation mechanisms, and we don’t know how to do that.
*Assuming the comomn adult male pattern of depression being expressed as anger holds true for boys as well.
The Talent Code (Daniel Coyle) makes three claims: that myelination is instrumental in learning, that skill is built by by methodically breaking down actions into component parts and perfecting them, and that these two facts have anything to do with each other.
Some background: your brain is made of nerve cells, which connect to each other and to other nerves outside the skull. We have only the foggiest idea what brain cells do, but we’re pretty sure the external nerve cells are for controlling muscle movement and reporting sensory data. Nerve cells communicate with each other by extending a long arm (called an axon) from their body to meet an axon from another nerve. Signals travel down an axon electrically, and between axons chemically. Like any electrical charge, nerve signals are subject to resistance and decay. To prevent this they are wrapped in myelin, a mostly fatty substance that insulates the axon.
I had never heard of myelin being involved in learning, and in fact it’s not on the wiki page, but deeper googling reveals that there is some fairly compelling research to back this up. Einstein had an unusually high number of glial cells (which, among other things, produce myelin). White matter (made up mostly of myelin and glial cells) volume in fine-motor-control areas in the brains of pianists correlates with self-reported practice hours. Most compellingly, mice prevented from producing new myelin are unable to learn a new task but maintain previous learning. And it makes a certain amount of intuitive sense that a substance that protects and speeds up nerves would be involved in learning. However, I don’t see anything here that tells us how a specific act of learning affects myelination of specific cells. Coyle’s explanation of this is so dumbed down I immediately want to trounce it, but as far as I can tell it’s a reasonable summary of the data for his purposes.
His recommendation to practice by breaking down a skill into component parts and refining them to perfection seems entirely reasonable to me. He cites a little bit of science for this, but mostly it’s just his observations of various talent hotbeds (The Spartak Tennis Club in Russia, KIPP schools, ). He believes these hotbeds stem from a combination of this cultivated practice and “ignition”, the ability to make a kid believe they can be successful at something. No doubt those are both helpful, but I don’t see any evidence that those factors and only those factors distinguish the talent hotbeds
This was originally going to be part of a longer series on several books with “talent” in the title, but there is only so much “intelligence is irrelevant, practice is everything” followed by absolutely no guidance on practice I can read. So, here you go.
Everything this book says is absolutely true. Mindfullness is awesome. Spending energy being angry at reality for not living up to your expectations is not useful. A calm acceptance of where you are now without attachment to the future is useful in almost any situation. But my primary feeling reading the book was “This is fine for you, but I’m going to get better, so I’m just going to go wait for that.” I told that to someone in the waiting room at the IV place who was probably suffering from something pretty serious*, thinking I was making a funny joke about how I had failed at zen, and she said “good for you, keep fighting.”
This captures a lot of the tension around health problems that are prolonged or chronic or ambiguous as to where they fall between the two. If you “accept your limitations” too hard you end up putting yourself in smaller and smaller boxes until there’s nothing left. If you don’t accept your limitations enough you push too hard and make yourself worse. How to Be Sick isn’t falling into those traps. It’s describing a third way, of zen acceptance that doesn’t overly narrow or widen your vision for the future because it’s not about the future. The problem is that this is hard to teach. The author had been practicing Buddhism for 10+ years when she fell ill, and most of the book feels more like describing the benefits or appearance of a mindfulness practice rather than how to achieve it. I did get one really useful technique out of the book, enough to justify all of the time I spent reading it, and I suspect that will be true for a lot of people so I do recommend it. It’s just not magic.
Although maybe it kind of is. I ordered the book from the library when my doctor looked at me and said “maybe being pain free isn’t a realistic goal for you and you need to redirect your energy to learning to cope with it.” But then I saw a specialist who told me that the damage was healing, would probably be finished in about a year, and in the meantime enjoy this pain medication that leaves you almost pain free. So I can’t rule out that this book actually is magic, and if you are at the point where you’re considering books with subtitles like “A Buddhist-Inspired Guide for the Chronically Ill and Their Caregivers”, you probably are going to try weirder things in your attempt to heal yourself. So give it a shot and please report back.
*I’m there to mainline protein because my teeth and stomach aren’t up to the task of eating enough to heal me, but a lot of people are there for debilitating but poorly understood collections of symptoms like fibromyalgia, or better understood but more terminal diagnoses like cancer. Nothing makes me you feel grateful for your health after having dead bone scraped out of your jaw like seeing an eight year old get cancer treatment.
Jezebel (via NYT): “Girls Outscore Boys on Math Tests, Unless Teachers See Their Names” New York Times: “How Elementary School Teachers’ Biases Can Discourage Girls From Math and Science” Study Abstract: “We’re going to skip explaining how we proved gender bias and just talk about its effects”
Actual Study (no public link): “Young Israeli girls outscore boys on anonymously graded national math exams but receive lower classroom grades, but eventually begin to underscore them in national exams as well. The size of the discrepancy in scores is positively correlated with discrepancy in teacher attitude reported by boys and girls. This pattern does not hold for English or Hebrew.”
I went in to reading this study pretty guns blazing, but it actually looks quite well done and robust. You could argue that the teachers and tests are evaluating different things and the teachers’ goals are not necessarily worse, but
Stereotypically, girls are better at pleasing teachers than boys. And that is in fact the pattern we see in Hebrew and English.
Low-biased teacher grades was correlated with a decrease in performance among girls in later grades (beyond that that would be predicted by low grades alone). The best case scenario is that the teachers are spotting some hidden weakness in the girls that the lower grade tests didn’t cover. Except…
Grade bias was positively correlated with negative student reports of the teachers attitude, and specifically discrepancies in the attitude reported by girls and boys.
So the actual study is pretty impressive, and astonishingly so for being in the field of education. Touche, Lavy and Sand. I also found it interesting that bias against girls was strongly correlated with the socioeconomic status of girls in the class as a whole, but not with any individual girl’s SES. E.g. having a poor girl from a large family with uneducated parents lowered the grades of other girls in the same class, regardless of their own status, which suggests all kinds of unpleasant things.
The popular reporting on this paper is less impressive. Jezebel flat out lies, implying that the same test was graded blindly and with the name (but no other data) available, which led to 100 comments asking how math grades could even vary that much, and 100 other comments saying “partial credit for showing work”. The New York Times isn’t quite so egregious but does describe the input as “The students were given two exams, one graded by outsiders who did not know their identities and another by teachers who knew their names.” That’s technically true, but implies that the two exams were much more similar than they actually were. I expect this kind of crap from Jezebel, but the New York Times shouldn’t have to sensationalize results that are already this interseting.
I talk to a lot of people in crisis chat who feel bad taking up my time, or are reluctant to seek treatment from a professional, or would pay for help but are reluctant to accept free help, because there are so many people out there with more serious problems. How serious their problem is varies: sometimes it really is a mild problem, sometimes it is years of horrendous abuse that is still technically not the worst thing a human being has ever experienced in the history of time.
The most useful response I’ve found is: “We treat people with sprained ankles even though there are other people with broken bones. Be honest about your situation and trust the doctor/therapist/charity to prioritize their resources appropriately.” Nothing works all the time, but I can’t think of a time it didn’t at least help.
A new study came out this week suggesting use of a particular class of drug after age 65 was associated with dementia. Here’s what you need to know.*
The study is retrospective, meaning it took people who developed the disease of interest and then looked backwards at their medications. Retrospective studies are prone to a number of problems, the biggest one being that even young people with healthy memories are crap at giving you their drug history over the past 10 years, and this is a study of people with dementia. The researchers dodged this by using an HMO database of the subjects complete medical history, which is a neat trick. The second problem is that retrospective studies can easily end up being painting the bulls-eye after they’ve fired the arrow. Mere chance dictates that if you track enough traits, any random subset of a population is likely to have something more in common with each other than with the rest of the population. If you use the traditional bar of statistical significance (5% chance of results arising by chance), checking 20 traits gives you an expected value of 1 false positive. To be fair, this study has a much higher significance level, and the effect was dose dependent, which is a very good sign that it’s legit. The authors heavily imply they deliberately studied anticholinergics rather than shotguning it, but without preregistration there’s no way to be sure.
Anticholinergics come in two forms: antimuscarinics, and antinicotinic. Short version: these work on different types of neuroreceptors, which live in different parts of the body and do different things . Every example drug they give is an antimuscarinic and of the classes of drugs they list, many have no antinicotinic members. Even if they technically included antinicotinics in the analysis, they would be such a small portion of the sample that their effect could be overwhelmed. So I don’t think you can apply this study to drugs like bupropion, which is an antinicotinic.
I don’t like the way they calculated total exposure at all. Essentially they counted the normally recommended dose of any medication as One Standardized Daily Dose. But those dosages vary wildly (even the examples they give span an order of magnitude), as do the particular drugs’ ability to cross the blood-brain barrier. The drugs are prescribed for a huge variety of causes, and what’s sufficient to stop incontinence has nothing to do with what’s sufficient to slow Parkinson’s. This oversight may cancel out with the fact that they created buckets of dosages rather than do a proper linear regression, in the sense that low-def pictures cancels out bad skin.
The obvious question is “but maybe the same thing that drove people to need anticholinergics increases the likelihood of dementia?” This study has a much better retort for that than most, which is that anticholinergics were prescribed for a variety of causes, and it’s unlikely they all correlate with dementia. I find that explanation extremely satisfying, except that they only evaluated the drugs as a single unit. Antidepressants make of over 60% of the total SDDs taken. The next most common is antihistamines at 17%. But since more than 60% of the population took at least one SDD, it seems likely that those were taken intermittently, as opposed to the constant drip of antidepressants. This leaves open the possibility that the entirety of the effect they attributed to anticholinergics was in fact caused by tricyclic antidepressants alone- and that the real culprit was depression. The obvious controls were to evaluate the anticholinergics separately, and to compare rates of dementia among TCA treated patients with those treated with other antidepressants.
The subtler version of this question is “what if anticholinergics prolong life, giving you more time to develop dementia?” I don’t see anything where they checked for that either way. They did ask for people’s perception of their own health, and that was negative correlated with TSDD, but if TSDD is correlated with depression it’s hard to know how to interpret that.
For all those criticisms, this is an amazingly strong result for a medical study**. No one study can prove anything (even if i think they had the data to do more than they did). It definitely merits further investigation (ideally some with animal models, so we can do the causality experiments that would be super unethical in humans), and maybe even behavior change in the meantime, although a lot of the drugs studied are already obsolete or second line. Plus it another piece of data that will help us figure out how to fight dementia, and that makes me really hopeful.