
The following is extracted from research I did for a client (which I’m sharing with their permission). An important thing to keep in mind while reading this is that the information was gathered to answer particular questions (Primarily “quarantine procedures for very risk sensitive, cost insensitive people”), and that biases what I looked at in weird ways. But I think it’s still much more useful for some set of you to have this information than not, so here it is.
The Tests
Symptoms
Of young, healthy people caught by prophylactic screening (typically contact tracing), 30-50% who test PCR+ will never report symptoms (in some cases these subjects are proactively screened for temperature, in others it’s not clear. Additionally, other studies have found that some percentage of people who report no symptoms will go on to develop CT lung anomalies). Additionally, most people who do develop symptoms spend several days being contagious before they develop symptoms. So symptoms are not a very good metric at all for determining if someone is infectious.
PCR
PCR tests look for specific viral RNA sequences and amplify them to make them easier to detect. They can vary in a number of ways:
- Specific sequence searched for
- Number of amplifications done
- Collection site and mechanism of sample
PCR false positives are quite rare, and typically have to do with sample contamination. False negatives are more common, and can come from a variety of sources:
- Covid was present but did not have the particular sequence searched for
- Did not do enough amplifications to notice effect
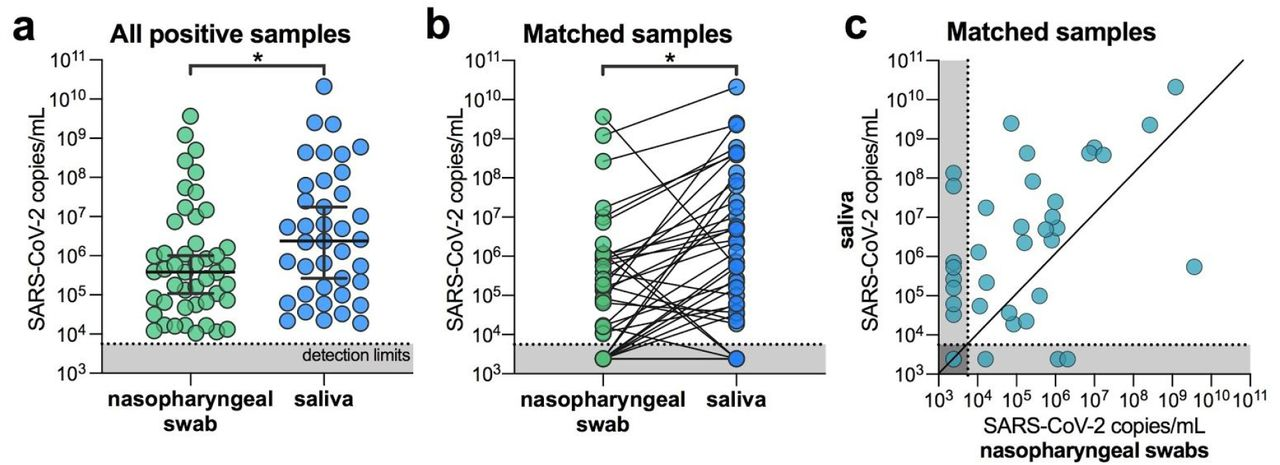
- Patient has covid but the particular site sampled does not.
How common are false negatives? That’s hard to define, because currently a nasopharyngeal PCR is what gets you diagnosed as having covid- if you fail that, you’re assumed to have one of the many things that produces similar symptoms. However, we can make some guesses.
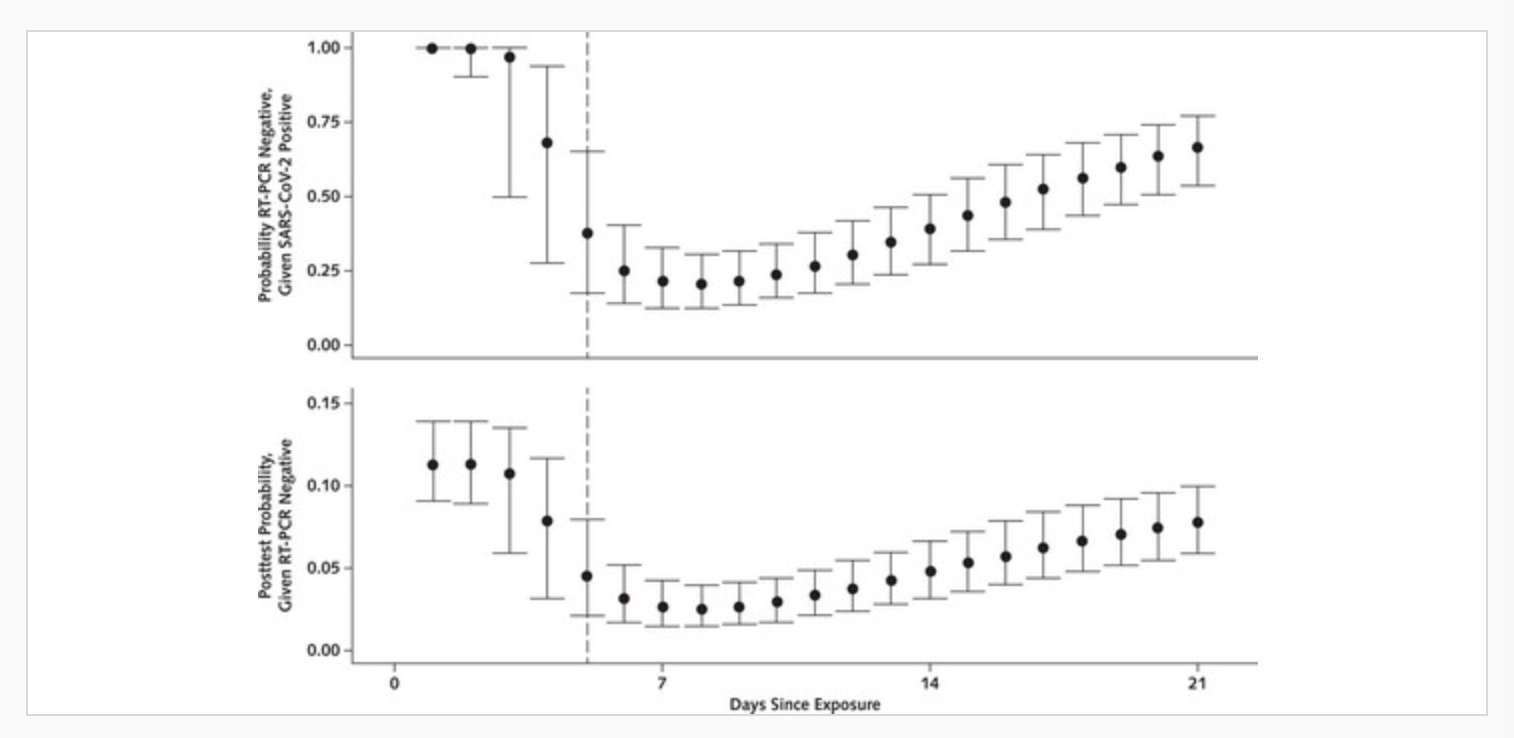
The following graphs show the calculated chance of testing PCR+ on a nasopharyngeal test on a given day after exposure, given frequent testing and an eventual positive result.
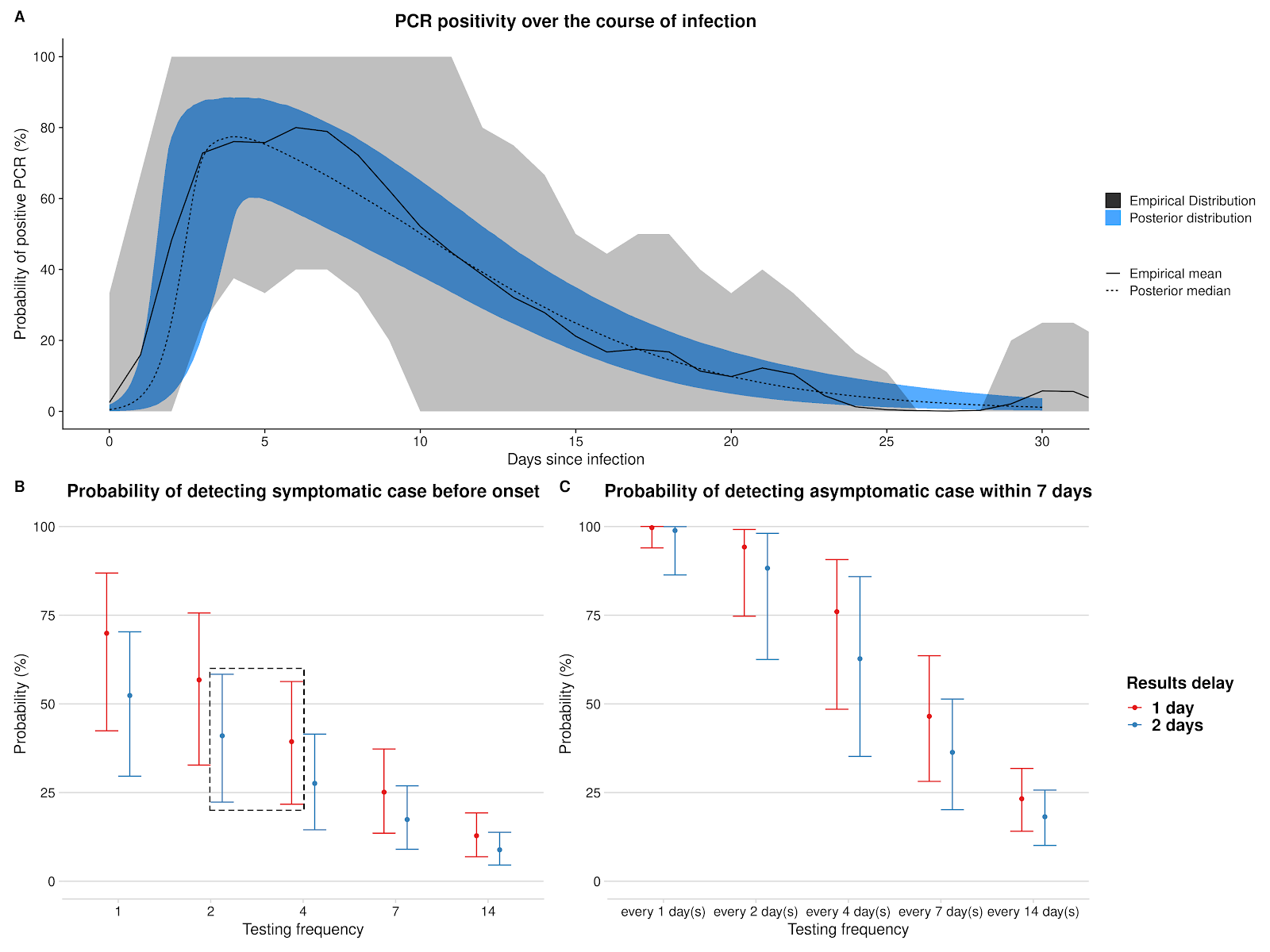
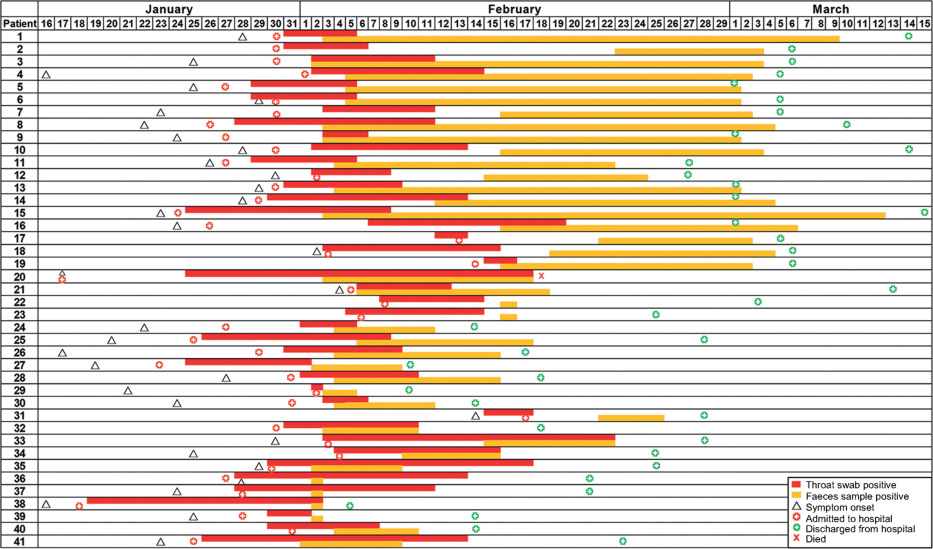
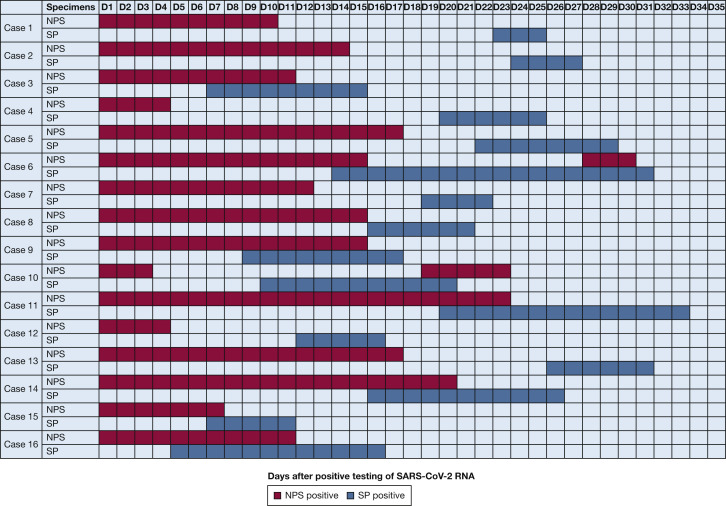
But that’s just for nasopharyngeal (NP) tests. Data on sicker patients (the only ones studied) show it’s possible to have a negative NP test while another area of the body (lower respiratory or gut) tests positive.
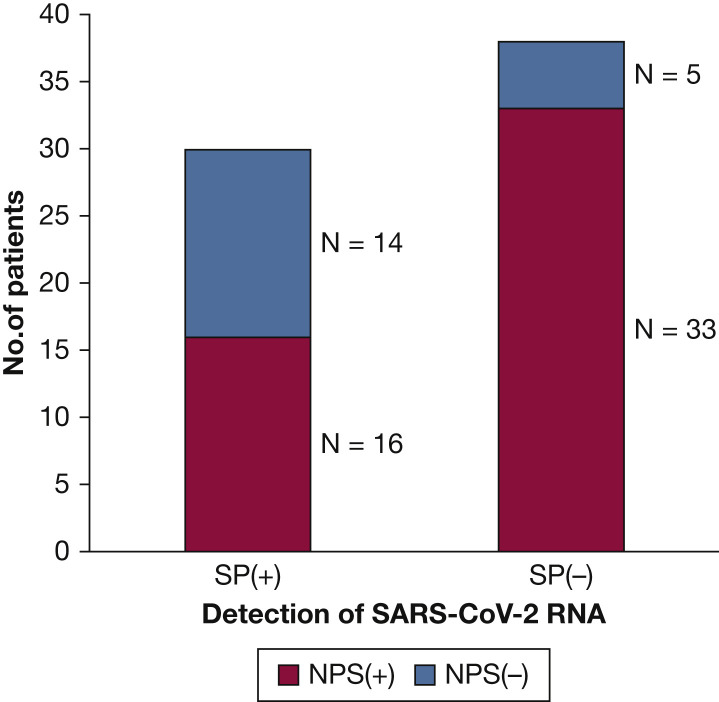
But these are all people who tested PCR positive eventually. What about people who get sick without ever testing positive? A very small study found that of 24 health care workers who developed positive antibodies over a 3 month period, 10 never had a positive PCR test despite being tested twice weekly. The paper offers multiple explanations for this, and I’m very reluctant to draw conclusions from such a small study, but it is concerning.
Antibody tests
Antibody tests look for an immune reaction to viral proteins. They can be negative when a person is contagious (because they haven’t formed a large enough reaction yet) and positive when they are not (because they successfully fought off an infection).
A reasonable question I have not investigated is “does an antibody+ test mean I’m immune?”
LAMP tests
Like PCR, LAMP tests look for specific viral RNA sequences and amplify them to make them easier to detect. LAMP tests go through many fewer amplification cycles, making them less sensitive but much faster: 30 minutes vs 2-3 days for PCR, plus the transit time for the PCR samples.
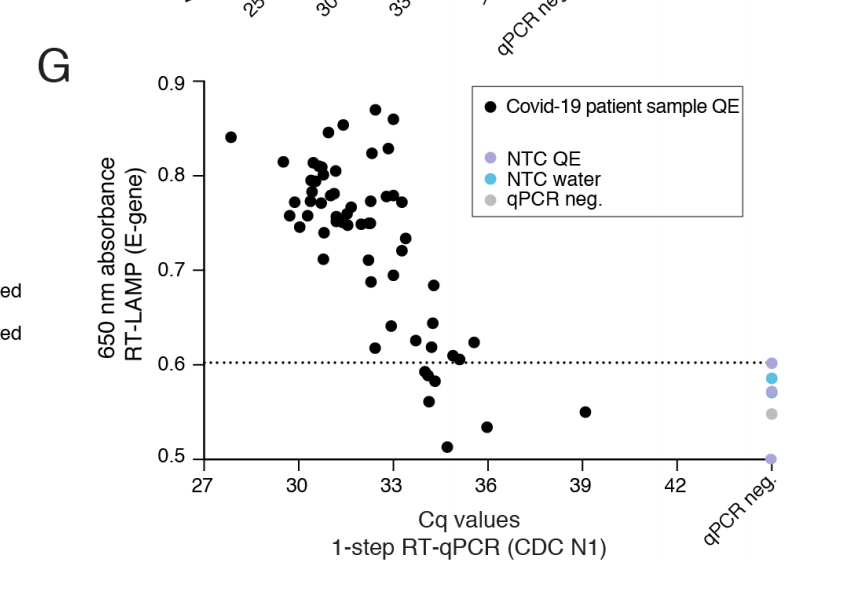
A LAMP test every three days is much more valuable than one PCR test, because catching the peak is much more important than the sensitivity. I’m not sure if a LAMP test taken today is more or less useful than a PCR test taken to give results today. I stopped digging into this because there were not yet any LAMP tests on the home market.
Antigen tests
Antigen tests look for specific viral proteins in a sample. There’s no amplification, which makes them less sensitive, but manufacturers report catching 88% of cases caught by PCR, so maybe this is fine, especially since you get results days faster?
The 88% sensitivity number is much, much higher than you see in literature (which is something like 20%-50%), I assume because they used more abundant samples. There’s some controversy over whether that’s because many PCR positives are driven by dead virus, in which case the antigen test returning a negative result is a feature, not a bug. This may well be true, however at least one study was able to culture live virus from a PCR+/antigen- sample, so it’s not foolproof.
Of the studies looking at antigen tests, all that I found either started post-symptoms, or took a random sample of people showing up at a sampling site. None were in a position to determine how good antigen tests are as an alarm system for catching an early infection (as opposed to diagnosing symptoms or determining when someone has ceased being contagious)
However antigen tests return results in minutes, while PCR tests take 2-3 days to complete not including shipping time. Given how quickly covid multiplies, it’s possible that an antigen test now is more sensitive than a PCR test from four days ago, especially if the exposure occurred in the intervening time.
What do any of these mean for contagiousness?
That’s a good question, which with the exception of asymptomatic spread can’t really be answered without human challenge trials, which the entire world declined to do. I would be surprised if any of these tests’ thresholds lined up perfectly with the threshold of infectiousness, because there’s no reason to expect they would. I expect culture tests to be much closer, but still not necessarily exactly on line (plus AFAIK they’re not available for diagnostics, even through a doctor). Given that I asked…
How long do I need to stay in quarantine after potential exposure?
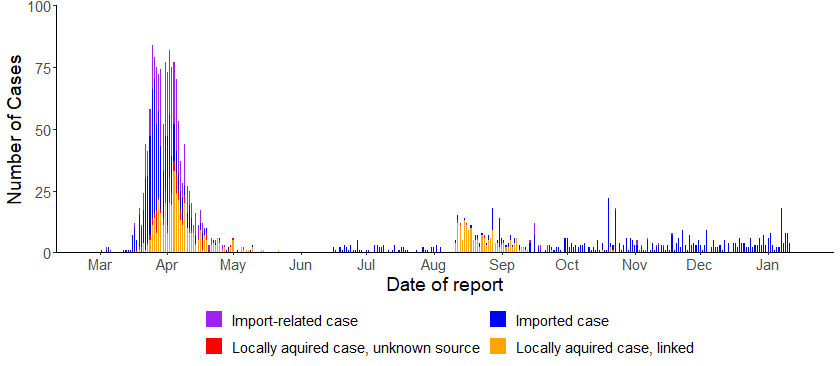
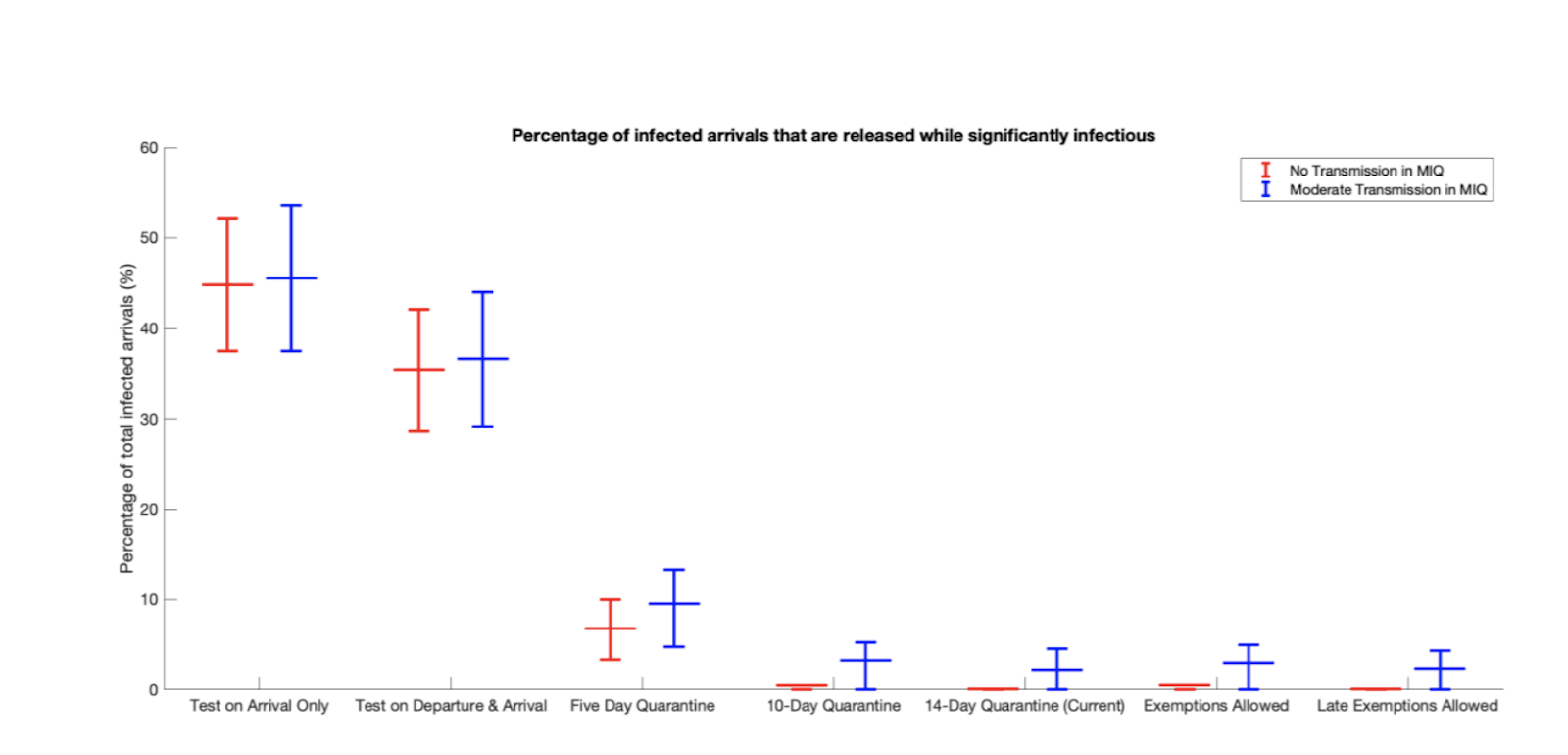
The best data on this is from New Zealand, which has a very strict isolation policy for entrants: 14 days isolation, with PCR tests on days 3 and 12 of isolation (a pre-departure test is required only if you’re coming from the US or the UK). By my earlier estimations, day 3 of isolation is already likely to be past the peak of detectability, unless travellers were exposed right before they left. Nonetheless, New Zealand reports only a handful of import-related covid cases after this policy kicked in, and a model attributes those to people who caught covid in isolation (e.g., a couple who shares a hotel room and one partner gives it to other on day 4), rather than people who entered New Zealand infected.
I did look for similar data from other countries, but NZ had both the best quarantine and the best data.
So despite the tests’ low sensitivity, 14 days + a test at the end really does seem to be a long-enough isolation period.
Thanks to my original clients for funding this research, and my Patreon patrons for contributing to the cost of preparing this for publication

Do all PCR tests take 2-3 days? It seems like it could theoretically be less:
“Typically, a PCR test takes six hours from start to finish to complete,” said Kelly Wroblewski, director of infectious disease programs at the Association of Public Health Laboratories.
https://khn.org/news/what-takes-so-long-a-behind-the-scenes-look-at-the-steps-involved-in-covid-19-testing/